
More on the miraculous new weight-loss drugs; Causes of the obesity epidemic; Support group; Fewer heart problems; Access disparities; Aspartame
Continuing where I left off in yesterday's e-mail, here's the rest of the e-mail I sent recently to my new personal e-mail list to follow the miraculous new weight-loss drugs (if you wish to join it, simply send a blank e-mail to: weightlossdrugs-subscribe@mailer.kasecapital.com)...
1) I asked my team of experts: "What's caused obesity to run amok in recent decades? Is it that food engineers at fast food chains and consumer food makers are designing foods that trigger the addiction?"
Dr. Jason Fung replied:
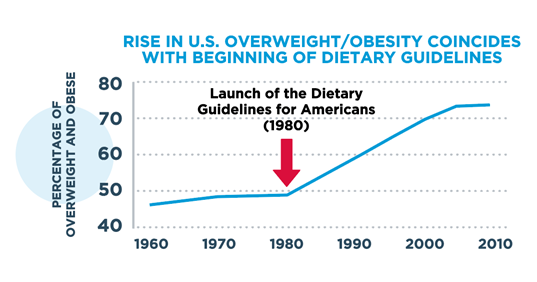
Good question, Whitney. Looking at obesity in the USA, we see this.
The slope of the line clearly changed with the Dietary Guidelines, which were important for several reasons. First, it was the first time that the government "backed" a specific diet.
Second, the focus was to lower dietary fat to reduce heart disease and there was no consideration of obesity which, at the time, was not a big issue. There is no evidence that lowering dietary fat reduces heart disease, as these guidelines have all been rescinded in the last few years.
However, in order to reduce dietary fat, the government encouraged 55-60% carbs, which were not broccoli, but mostly white bread, pasta and rice – not exactly slimming foods. Also, government encouraged the development of highly processed foods (to process out the fat, unfortunately by adding more sugar). So the real rise of processed foods changed significantly with the Dietary Guidelines – more sugar, more additives, less fiber, more refined carbs – all considered good, because they were low fat.
This was also an era that we thought we could make a better breast milk (formula) than breast milk. Seems stupid now, but physicians needed a massive public health campaign called 'breast is best' to convince people to go back to breast feeding.
Perhaps the dietary guidelines had nothing to do with the rise of obesity, but it seems too much to be a coincidence.
Dr. Kevin Maki added:
The prevalence of obesity in the U.S. was fairly stable through the 1970s and then took off starting in about 1980. There have been many changes in culture and lifestyle that may have contributed. I think that changes in the food supply have likely played a role. However, there are a myriad of other issues as well.
Physical activity is lower than it was in the 1960s, screen time and other sedentary behaviors are up, intakes of refined starches and added sugars in highly processed foods with high energy density (kcal per 100 g consumed) are also up. Snacking between meals has become much more common than it was in earlier decades and where, when, and how Americans eat has evolved in ways that may promote overconsumption. Anxiety and depression are more common now than in past decades, particularly in adolescents and young adults. Food is used by many for psychological/comfort reasons when lonely, bored, or anxious. All of these factors and more may have played some role and there is no clear single cause.
The daily energy imbalance needed to explain the obesity epidemic is very small, as outlined by Kevin Hall from the NIH and colleagues below (a persistent imbalance of only 7 kcal per day can explain average weight gain – see excerpt from this Lancet paper, Quantification of the effect of energy imbalance on bodyweight). Obesity appears to be preventable but very difficult to treat once present. Kevin Hall and his colleagues conducted assessments of participants in The Biggest Loser show and this link is to a slide deck that outlines their findings. Some of the same material is covered in this webinar. The summary from the slide deck is as follows:
- The body resists weight loss and promotes weight regain via slowing metabolism and increased appetite
- Long-term maintenance of lost weight requires ongoing support and persistent effort
- Increased physical activity may be especially beneficial for maintaining lost weight, in addition to its overall health benefits
- Reengineering your food environment may help facilitate maintenance of lost weight
- Less ultra-processed foods with lower energy density
In my view, pharmacotherapy will have an important role to play in obesity management, but drug therapy needs to be paired with lifestyle intervention involving a healthy diet, exercise (aerobic and resistance), adequate sleep quantity and quality, stress management, and psychological/behavioral support.
Rich Weil commented:
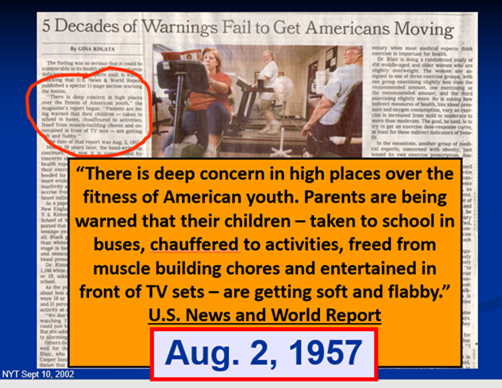
I show this slide frequently in our weight loss program. Published in the NYT in 2002, it shows as far back as 1957 that the problem already existed:
I once read an excerpt from a book from the mid 1880's (not 1990's) that reported gluttony and sloth were already problems, comparing residents of France to the United States. Again, that was in the 1800's. There is evidence for the problem in the early part of the 20th century, and the President's Council on Fitness started in the Eisenhower administration in the 1950's because they were concerned about the lack of fitness in our school children and the potential for an unfit for combat armed services vis a vis the Red Scare.
I have read Kevin Hall's work, and heard him speak many times. He is a brilliant guy, but a physicist, not a clinician, and I have used his calculations to estimate how much weight someone would lose based on multiple variables. When I applied it to the real world of our weight loss program population, it wasn't close. But the points from the webinar that you outline are good ones, but they don't explain the whole story. I've been at this 40 years, weight loss and preventing regain, especially in the real world, when people go to work, deal with all the problems of daily life including sick parents and children, financial stress, illness, genetics, epigenetics, and so much more, all which make obesity a serious and major multi-factorial problem to say the least. I have constructed a list of more than 32 factors that apply to a model of obesity that I teach, and the list grows.
All the reasons you post below about causes of the obesity epidemic are true, and of course there are many more variables, but as I said, this problem has been around much longer than most people think. You might even ask why BMI was developed in the 1830's through the 1850's, what was the concern then? And then the modern version in the early 1970's by Ancel Keys.
I've already mentioned it multiple times in these emails, the weight loss meds are game changers. Finally we have something that side-steps the bias that people with obesity are weak-willed, lack discipline, and have character flaws, and deals directly with the neurobiology of the brain and many other factors including appetite regulation. I take extreme exception to individuals, including physicians and investigators, who complain that you might have to take weight loss meds for life. So what? People take all sorts of meds for life for many medical conditions, and you don't hear people complaining about that. What's the problem with taking a medication for life that treats the chronic disease of obesity? And you might only need to take it once a week. And wait for the new medication from Lilly in phase 2 that looks even better than Mounjaro.
And as I mentioned previously, none of these weight loss medication articles in the media are enlightening me or many of our colleagues to the problems or solutions. They sensationalize the problems and make things worse.
Dr. Maki added:
Agree. People take medications to prevent heart attack and stroke for decades such as those for lipids and blood pressure. Effective weight loss will lessen the need for these. Like other chronic diseases, obesity requires medical management, including behavioral and lifestyle support, and medications will play an important role for many. While obesity is much more common now than it was in the first half of the 20th century, it was present in 10-15% of the population even then. I hope that the availability of effective drugs will help to change the views of healthcare professionals so that obesity is viewed more as a chronic medical condition rather than reflective of deficiencies of character and discipline.
2) By the way, Rich is offering a new weight-loss medication support group for individuals who are taking weight loss medications or considering it:
With the popularity of the new, effective, and safe weight loss medications, we have decided to start a new weight loss medication support group for individuals who are taking weight loss medications or considering it.
We believe that with the wide-spread use of these medications, and the rapid and large amounts of weight loss they cause, individuals will experience emotional/psychological and physiological changes that are new and can be unnerving, especially if you have had obesity all of your life or all of your adult life.
With the speed and amount of body weight changes that these medications are causing, there are many issues that need to be addressed with authoritative and accurate information, and with group support facilitated by health-care experts, especially professionals who have weight loss experience. Some of the many issues that we will cover in the group are:
- Dealing with not feeling hungry, maybe for the first time
- Dealing with feeling full, maybe for the first time.
- Shopping for new clothing at a brick-and-mortar store and not online.
- Reducing or eliminating the "noise" about food in the brain such that obsessing and cravings are no longer an issue.
- Learning how to plan what to eat and setting new and different kinds of food plans.
- Leaving food on your plate.
- Losing interest in food.
- Compliments about your new appearance.
- Side effects of the meds.
- Being able to physically move easier.
- Addressing body image issues such as fitting in seats that you never thought you could fit in before; simply taking up less space; having your picture taken, and more.
- How to navigate the insurance system and problems with acquiring the medications.
- All the benefits of learning about lifestyle changes to complement the use of the meds. The drug companies recommend diet and exercise to complement the use of the medications, and it's been our experience that people taking the medications who lose the most weight are consistently participating in many lifestyle changes including regular exercise and attention to healthy diet choices that are an intrinsic part of our program.
- And many more emotional and physiological issues that are new to individuals who have lost as much weight and as quickly as the new weight loss medications are causing.
We are waiting to set the start date depending on interest, but interest has been high, so we are ready to move on this in the next 2-3 weeks.
Our website is www.FitsMeHealth.com You can reach me at this email address if you have questions:
Please email me at Rich@fitsmehealth.com if this is a group you are interested in joining.
3) The paper was published in the New England Journal of Medicine on September 21: Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity. Here's the summary:
Novo Nordisk's (NVO) anti-obesity drug Wegovy also eased the symptoms of a common form of heart failure in patients who also have obesity, according to results published online in the New England Journal of Medicine. The patients who took the once-weekly injection for a year reported improvements in fatigue and shortness of breath, and found they could walk longer distances, all while losing an average of 13% of their body weight.
Dr. Maki commented: "These results are as I would have predicted. I expect the results from the SELECT trial to be presented and published in November in conjunction with the American Heart Association meeting."
Rich added:
I agree. I also would have predicted the same. Not really that much of a surprise. As an aside, it used to be we told patients with heart failure not to exercise, or do it very, very lightly. Now that's all changed. Exercise has been shown to improve heart function and quality of life in heart failure patients. With medications such as semaglutide on board, profound weight loss, and regular exercise, this combination is going to make an enormous difference in health and quality of life for many individuals, with many different medical conditions, and not just heart failure.
Dr. Maki wrote:
Spot on, Rich! I am in the middle of a project to look at the effect of weight loss on risk for chronic kidney disease (in Dr. Fung's wheelhouse). The list of conditions associated with obesity is long and I am hopeful that we will see benefits for many. A partial list includes heart attack, stroke, diabetes, kidney disease, high blood pressure, heart failure, arthritis, depression, sexual dysfunction, and urinary incontinence.
4) This New York Times article triggered a discussion among my experts: The N.Y.C. Neighborhood That's Getting Even Thinner on Ozempic. Rich wrote:
NYC obesity and diabetes maps by zip code, poverty, and socioeconomic status, have always shown what you expect. The poorest neighborhoods, and people of color, always had the highest rates. The upper east side of Manhattan, where there is a high concentration of wealth, always showed, and still does, low levels of obesity and diabetes. Hopefully what happens is that the medications become affordable and available to everyone, and not just those who can afford it, or have employers or insurance that covers it.
This article reminds me of an expression we used decades ago that applied, in particular, to wealthy women and socialites on the upper east side of Manhattan as "social X-rays." One of the problems is that individuals who have just a few pounds to lose are taking these medications that are not indicated for them, and creating shortages for people who need them. Let's hope Medicare gets on board, and Medicaid contributes more than it already is doing, and that overall the medications become more financially accessible and available. I was interviewed recently about the meds, and the interviewer asked me if this is the end of obesity. I told him that that might be a slight stretch, but it certainly is for people who are fortunate to have access to them and continue to take them. I've never seen information about a medication reach the consumer faster than these meds.
Dr. Maki added:
I am hopeful that information about benefits regarding heart attack, stroke, and heart failure will prompt wider availability of these agents to people who are not wealthy. The largest burden of obesity-related diseases is among racial and ethnic minority groups and those with lower socioeconomic status.
Rich replied:
I've never seen the information about a medication, for weight loss or any other condition, reach the consumer as quickly as these weight-loss meds have, so maybe there is some hope that the message will get out to a wider audience. And of course, the issues we have already discussed such as availability, education of doctors and the public, use of the meds off-label or when it's not indicated, and a myriad of other issues.
Dr. Fung chimed in:
Precisely why I find it unfair that doctors and the media push Ozempic so hard while ignoring interventions like intermittent fasting that can benefit everybody, and not just the rich.
At physicians' conferences the lectures dedicated to Ozempic compared to fasting are about 1 million to one, if that.
I asked: "I agree with you about the benefits of intermittent fasting (IF) – I've tried it myself – but it's hard and I think only a small fraction of people could/would do it, even if doctors, leaders and the media pushed it."
Rich weighed in:
IF is to some degree a restrictive intervention, even though it seems to be easier to follow for some people than other dietary changes, but if it's restrictive, which we have observed, then it will not be sustainable. There are times where I have counseled patients to eat only at specific times of the day to get control over food and cravings back, but again, these sorts of restrictions mostly lead to rebound.
As effective as IF can be, and we have seen that to be the case, and recommended it for as long as it has been around, with success, but I don't think in the long run, that IF will be able to compete with the medications. There are simply too many mechanisms of action with the meds, including the brain and other organs, that helps regulate appetite, which is very complex. IF can't do all of that, and again, it can be viewed as restrictive for people, and once they start rebounding, that rebound turns into lapses or relapses for physiological and psychological reasons.
We won't stop recommending IF, especially for patients who don't want meds, but a comparison between the two is a stretch.
5) My mom is bugging me about my Diet Coke consumption (as I sit here drinking one!), citing this study to link it to a few hypomanic episodes I've had in the last dozen years: Neurophysiological symptoms and aspartame: What is the connection?
I asked Dr. Maki what he thought, and he replied:
I have done studies with various high-intensity sweeteners for decades. I am not an expert in the neurobehavioral aspects, but I know that many of the claims made for cardiometabolic effects and obesity have been based on very weak evidence, mostly from studies in animals, and on theoretical concerns. I remain unconvinced and the results from the studies I have done do not support adverse cardiometabolic effects.
Also, one has to compare even potential adverse effects to those from added sugars, which appear particularly bad, especially when consumed in beverages. I think that limiting intake of high-intensity sweetener intake to some reasonable amount (say, 1 serving of diet soda per day) is a good way to hedge. I have a history of drinking a lot of Coke Zero and have tried cut back with flavored carbonated water as an alternative. Personally, I have observed no differences in how I feel or behave with and without high-intensity sweetener consumption and various metabolic measurements have shown no differences for me. I can say that I enjoy Coke Zero much more than carbonated water!
I can't rule out the possibility that some individuals may have adverse responses. I remain very skeptical of claims of adverse effects but keep an open mind and hedge my bets by limiting consumption. I am much more concerned about added sugars, and to a lesser extent, refined starches, than I am about reasonable levels of consumption of diet sodas.
6) Other articles of interest:
- The Company That Defined Dieting Is Sorry It Told Us to Have More Willpower
- How Stress Leads Us to Reach for Comfort Foods
- Amgen Could Get a Piece of the Obesity Market
Best regards,
Whitney
P.S. There's still time to register for today's investment briefing I'm holding with investing legend Alex Green, where we're sharing the details on a chance to make 5 to 10 times your money through a huge turning point in the market most people will never see coming... as the result of a major new event taking place later this month in Orlando, Florida.
Put yourself on the list to receive today's briefing right here.
P.P.S. I welcome your feedback at WTDfeedback@empirefinancialresearch.com.